Building a positive relationship with food and your body
For an accessible version or to translate, visit:
https://tinyurl.com/2nwt9w32
Scan to view online

Avoidant Restrictive Food Intake Disorder
Parents and Carers
 Download
DownloadTrack your progress

Understand how challenging
it can be to have a child with ARFID
We want to let you
know that this is
NOT YOUR FAULT
You are doing the
best you can, with the
knowledge you have

We also know that being part of a supportive group is very
important, so we encourage you to join one – BEATM and
ARFIDAWARENESSUK
Our aim with the following slides is to give you
more information on ARFID
We always like to explain that the eating can’t be “fixed”.
We like to think of it as a work in progress, especially if there are
other difficulties around (i..e anxiety, other diagnosis,
trauma)
What is ARFID – Avoidant Restrictive
Food Intake Disorder?
APPARENT LACK
OF INTEREST
IN EATING
FOOD AVOIDANCE
BASED ON SENSORY
CHARACTERISTICS OF
FOOD
CONCERN ABOUT
AVERSIVE
CONSEQUENCES
OF EATING

- 1 Significant weight loss (or failure to gain weight or faltering growth in children)
- 2 Significant nutritional deficiency
- 3 Dependence on oral/enteral feeding
- 4 Marked interference with psychosocial functioning
What ARFID is NOT

Who can have
ARFID?

Anyone of any age can
have ARFID
People with ARFID can
be any weight
ARFID can be long-term or
come on suddenly
ARFID often co-occurs with autism, ADHD, or other learning difficulties
THINGS YOU MIGHT HAVE NOTICED….
- Sensitive to smell, look, taste, texture or all together
- Not feeling hungry, forgetting about eating, feeling full very quickly, not “liking” to eat, no interest in food or all together
- Fear of eating because it might cause vomiting, choking, gaging or all together
- Anxious temperament

NEGATIVE FEELINGS ABOUT FOOD
- Fear of new foods and not wanting to try new foods
- Smelling the food before trying
- Thinking that it won’t taste good anyway so it might be better not trying
- Thinking the food will make them sick/ vomit/ choke
- Not wanting to eat a food once eaten because it caused some reaction in the past (allergy, vomit, choke)
HEALTH CONSEQUENCES
- Weight loss
- Reduced hunger
- Vitamins and minerals deficiencies
- Difficulty to gain weight
- Gut symptoms (i.e. upset stomach)
- Feeling full quickly
- Constipation
- Not getting taller
ACTING DIFFERENTLY AROUND FOOD
- Not eating at the dining table
- Finding it difficult to eat at school
- Not eating in front of other people
- Not feeling hungry / not being able to say they are hungry
- Feeling uncomfortably full
- Sensitive to changes on how food looks
- Noticing small changes in food and its packaging (i.e. if the package has a different colour)
- Getting angry when they are forced to eat
NOT helpful things to do
Hiding foods they don’t like – they will find out and will impact
their trust in you
Letting them go hungry – they will enjoy not having to eat and this will impact
even more their lack of hunger
Pressure to eat or finishing on time – it will increase anxiety and it will not make them eat faster
Not giving their preferred food - They won’t start eating other foods if you limit the amount of preferred foods
Having the idea of “good” and “bad” food – food is food and if they are only managing a few foods, this is ok for now

Expectations
We all know that as
parents, we would like to
eat a good variety of
foods and eat in
restaurants but the
reality is that
sometimes this will take a
long time to happen
So adjusting our
expectations and
thinking about how
important the “baby
steps” are is
essential

We do have successes but we also have “good enough”
So have a think about what success looks like…

Anxiety curve

The graph shows 3 lines:
-
Green – expected anxiety with new situations – anxiety starts lower, during the situation it goes higher and over time, it reduces as you know what to expect
-
Yellow – expected anxiety when you avoid situations – anxiety starts higher as you know you are avoiding a situation. Over time, the anxiety remains really high as there is no opportunity to exposure ourselves to new situations
-
Red – expected anxiety when you expose yourselves to situations – anxiety starts lower, goes up when faced with a new situation, but then the more you expose yourselves, the lower anxiety will be
Why preferred foods are important
The preferred foods are often calorie dense food so you can eat more
without feeling full so quickly
That it is for a short period of time for weight gain (if needed)
OR to increase interest about food again
The preferred foods tend to be “processed foods” (in the sense of coming from
a packaging) this is because they know what to expect from that food, there is no
surprises. This is the same reason why they tend to be brand loyal.


Why preferred foods are important
Child doesn’t eat all day at school or eat very little. They are very tired, difficult behaviour try to eat, but feels full very quickly continues to feel hungry
It is important to explain that there might be other hunger signals rather
than a rumbling stomach, i.e. headache, moody, irritable, sleepy, lack of
energy, lack of concentration, more sensitive, hyperactive
Energy levels

Child doesn’t eat all day at school or eat very little. They are very tired, difficult behaviour try to eat, but feels full very quickly continues to feel hungry
It is important to explain that there might be other hunger signals rather than a rumbling stomach, i.e. headache, moody, irritable, sleepy, lack of
energy, lack of concentration, more sensitive, hyperactive

Energy levels
That is why eating regularly is SO IMPORTANT
Some strategies:
Talk to school about it and ask them to allow preferred foods at school
Lots of children will tolerate drinking at school – think about fruit juice,
smoothies, hot chocolate, milkshake
See if school can provide a quiet room for them to eat, the
dining hall tend to be quiet overwhelming
Keep a timetable and planned meals
Use of alarms to remind them to eat

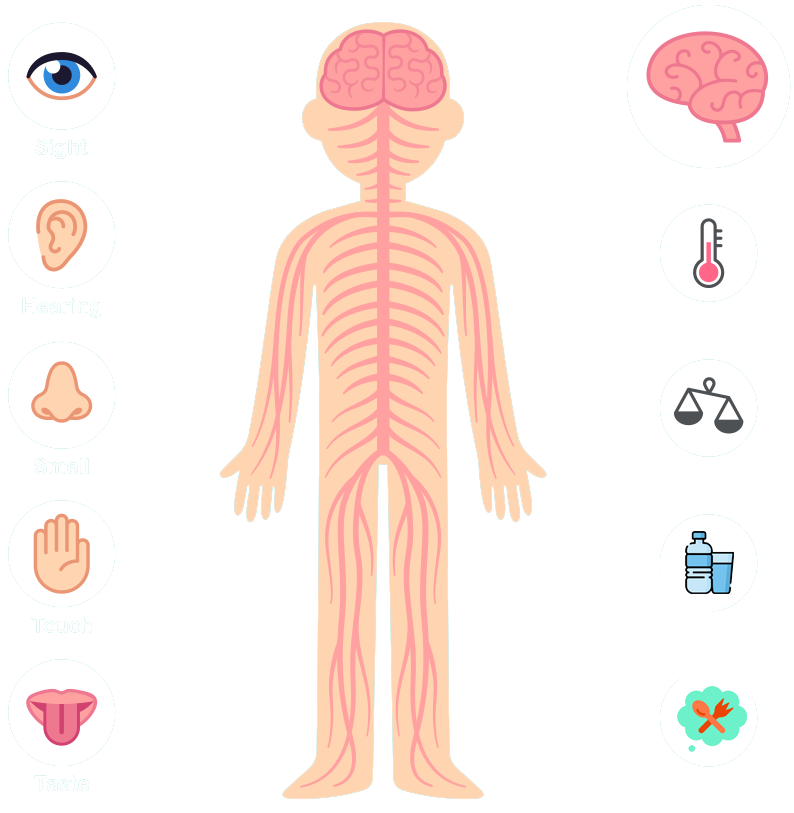
Interoception
Interoception is called the
8th sensory system
It is the ability we have to read our internal body signals
when we are hungry, when we are thirsty, when we need
to go to the toilet, if we are hot or cold
Most children, especially those on the spectrum, struggle to recognise these signals and therefore find it difficult to know when to eat and sometimes when to stop eating
Interoception

Hypersensitivity X hiposensitivity
-
 Heightened sensitivity to the internal sensations in the body.
Heightened sensitivity to the internal sensations in the body. -
Hunger may be extremely distracting and even painful
-
Extreme emotional responses- Fight /flight or freeze
-
Difficulty maintaining attention to tasks
-
Obesity may be related to hypersensitivity to interoceptive
-
Signals of hunger resulting in increased food cues
-
Overactive food reward signals
Less sensitivity to
the internal
sensations
in the body
They may never feel full after eating – or they may never feel hungry in the first place
Crave more
intense input
Obese individuals might be less
sensitive to
interoceptive
signals of fullness than to seeing
appetising food

Other strategies to help with
overstimulation/ under stimulation
Overstimulation:
-
Glitter jars
-
Stress balls
-
Fidget toys
-
Pop toys
Under stimulation:
-
Massage cubes
-
Wobble cushions
-
Weight blanket (seek further advice for this)
-
Toys that vibrate
This is not an exhaustive list, so create
one with your child

How to manage others expectations
including extended family
We know that the pressures from the
extended family and a close circle
of friends has a huge impact on how
parents feel
Involve extended family members as much as you can, giving them a role to play in supporting the child – exposure and removing pressure
Acknowledge that they may not be able to understand but accepting that the child needs support is the main thing


The importance of self-care
We all know that can be exhausting to look after
a child that has ARFID and possible other complexities
We always encourage parents to think about taking a
moment to enjoy themselves, to do something that they
can relax, to be better able to manage difficult situations
Also having a journal/ diary where you can express your feelings can be very helpful
We also know that when parents are anxious, the child will be even more anxious
This can be as simple as simple as taking a bath, having a cup of tea, going for a walk

Things that can impact eating – especially when they are young
1: Postural Stability – the
ability to control the body
position in space for the
purpose of movement and
balance
2. Sensory needs -
difficulties receiving and
responding to
information from
their senses.
3. Oro-motor skills -
awareness, strength, co-ordination,
movement and
endurance of the mouth; jaw, tongue, cheeks and lips
4. Experiences – related to food
that could have impacted
the ability/willingness
to eat

Postural stability
Children with Low Muscle Tone May…
Slouch while
sitting
Slide out from
underneath
tables/trays
Prop when
sitting
Not self feed
Like to walk around
and eat
Prefer to stand
and eat


90-90-90 position

Wrong position

Right position

Sensory needs
Eating is a multi-sensory process involving the co-ordination of eight systems:

Sight: changes with every chew.


Sound: changes with every chew (different consistency)


Touch: changes with every chew (texture is different)


Taste: changes with every chew (molecules are broken)


Smell: changes with every chew (molecules are broken)


Proprioception: changes with every chew (pressure is different)


Balance: changes with every chew (head shifts)


Interoception: sensation of movement in oesophagus changes, stretch on stomach and appetite changes

What can I do to help my child?
Understanding that eating can be a difficult process as it includes all our senses
Understanding and think about the 32 steps to eating
Managing my own anxiety, so I am better able to handle challenging situations
To try and have a curious approach about the difficulties my child is experiencing
(i.e. “I can see you find eating at the table difficult, what do you think might be happening? What can we do to support you?”)

How to approach it?
Food Chaining is a way of taking a food that your child likes and slowly adding subtle variations to this food until they can tolerate new ones.
How could we work with that?







Food chaining – other ideas
FRIES TO CARROTS
Learning to eat new colour

French fries

Sweet potato fries new colour

Butternut squash fries same shape & colour

Steamed carrots new texture

Roasted carrots same shape & colour

Roasted b.squash new shape

Food Chaining involves gradually and systematically diversifying the foods a person will eat.
For example:
You begin with a food that is currently accepted. You then consider what can be tolerated in relation to change i.e. colour, brand, texture, shape.You then identify a new food to try based on what can be tolerated. This new food is then introduced. This then restarts the process.
POTATO CHIPS TO BANANA
Learning to eat new colour

Potato chips

Plantain chips

Banana chips

Banana

Frozen banana slices

Freeze-dried banana

VEGGIE STRAWS TO GREEN BEANS

Veggie sticks

Green only

Snap pea crisps

Green beans

Raw green beans

Freeze-dried green beans
@Feedingpickyeaters
CHICKEN TO FISH
Learning to enjoy more protien

Fave nuggets

Fave nuggets

Fish sticks

Baked white fish

Fried white fish

Fish patty
Messy Play
- The child does not have to eat the foods presented to them
- It is about exploring food with the child
- It is about sharing an experience with the child, not to the child.
- Regularly reassure the child that they are “ok”
- It is about getting messy – wash hands at the end
Use different food characteristic,
for example:
- Large dry foods
- Medium dry foods
- Fine dry foods
- Wet drinks
- Sticky foods

Progress through food texture


6 Steps to Eating
Visual

What does it look like?
- What is the colour?
- What size is it?
- What is the appearance?
Touch

What does it feel like?
- Is it wet or dry?
- Does it feel cold or hot?
- Does it feel bumpy or rough?
Smell

What does it smell like?
- Is it weak or strong smell?
- Is it a nice smell?
Taste

What does it taste like?
- Does it have a strong taste?
- Is it sweet or salty?
- Is it spicy?
Texture/Sound

What is the texture like?
What sound makes in your mouth?
- Does it feel loud when you chew it?
- Is it crunchy?
- Does it get soft quickly?
*Not expected to eat, it is ok to spit it out
Swallow

Any other sensation?
- Any other sensation?
*Smell mouthful is ok and gradually increase quantity- Emphasise that they are not expected to eat the food!!!
- Outside of mealtimes
- To try and stick to a routine – so they know what to expect
- To use different place to practice
Other strategies
- Fade in - adding small amounts of food they don't like into food the like
- Add some spice – ketchup, curry, salt, honey, sugar
- Food chain –– try similar foods i.e. veggie chips with same format to potato chips
- Change presentation – salted x unsalted
- Deconstruct – break the food i.e. pizza – try with a piece of bread add tomato sauce add cheese…
THEY NEED TO AGREE WITH THESE STRATEGIES!


Examples of targets
To explore 5 foods through touching, with utensils, fingers or whole hand during therapy block.
To explore all foods offered through touching, with utensils, fingers, or whole hands, or tasting during the therapy block
To participate in routine (e.g. washing and drying hands, tidying up) with minimal adult support
To explore 2+ pieces of equipment during sensory preparatory play with minimal adult support.

Long term treatment as it takes time to develop a new skill, need a lot of support from the parents/carers/family
VERY important to discuss parent’s expectations and what success looks like for them!!!
There is no right/wrong OR specific steps to get “there”…. Each child will work in a different way
Each step can take days, months…and sometimes years…. They may change their minds during the process
Depending on their presentation, they can “jump” stages (i.e. from square bread to bread and cheese) OR they will need more steps – always ask how they feel about it and explain what to expect
The new food should not be expected to be eaten straight away, sometimes is just about exposure
Think about the 32 steps to eating

Other things to consider
- We know that routine works well for most children, especially for those with ARFID
- Think about a visual timetable and possibly a visual meal plan
- Think about offering 2/3 options (maximum per day, so they also engage on this)
- Taking them to shopping and letting them chose some new foods
- Having a separate cupboard can be helpful sometimes
- Reward system – can be helpful with some children
- Distractions at meal times – can be helpful in some cases, but ideally is a working in progress to remove this so children can be present whilst they are eating
- To use a hunger chart, to help them track and understand their hunger signals
- Have your child be part of the meal where possible – helping to prepare, setting the table, or just bringing their own plate to the table
- Encourage them to serve others food, even if they are not serving themselves
- If possible, have a ‘learning plate’ in front of your child. They can serve a small amount of food on to this plate. There is no pressure for them to eat this food, but they can look/smell/touch/play with this food.
- Have meals together as a family where possible, even if you are eating different things. This gives the child opportunities to be around different foods.
- Have a familiar routine around mealtimes – wash hands, set table, eat food etc.
- Make sure your child is sitting in a comfortable chair (feet on the floor).

Hunger Chart
- 0
- 2
- 4
- 6
- 8
- 9
- 10
 really hungry
really hungry
 really full
really full
| Monday | Tuesday | Wednesday | Thursday | Friday | Saturday | Sunday | |
|---|---|---|---|---|---|---|---|
| Early Snack | |||||||
| Breakfast | |||||||
| Mid morning snack |
|||||||
| Lunch | |||||||
| Pudding | |||||||
| Afternoon snack | |||||||
| Dinner | |||||||
| Pudding | |||||||
| Evening snack |


My Reward Chart




Task
| SUN | MON | TUE | WED | THUR | FRI | SAT | |
|---|---|---|---|---|---|---|---|
WEEKLY GOALS |
DONE |
|---|---|



- Ongoing poor weight gain, weight loss
- Ongoing problems with vomiting
- Stunted height
- Vitamin and mineral deficiencies (are they eating foods from all food groups)
- Ongoing choking, gagging, coughing during meals
- Aversion/ avoidance of all foods in specific texture or food group


Putting pressure on them can increase their adrenaline, which can suppress their appetite and make them less likely to eat. Try to remain calm and positive at mealtimes.
This is to help you remain as relaxed as possible and keep anxiety low
Daily routine for feeding: try to stick to consistent times each day and if needed, create a meal plan together so your child knows what to expect
Mealtime routines: prepare (i.e. “lunch will be ready in 5 minutes”). You might need to have some calming activity: wash hands together, sing song, blow bubbles, sit at the table, clean up, wash hands, finish. Consider also using stress balls, tangle toys, weight blankets, anything that calm/help your child
Avoid negative comments (avoid words like ‘no’, ‘don’t’, and
‘naughty’.
e.g. throwing, refusing, gagging. Telling a child off
or making a fuss often increases that behaviour.
Instead try a sticker chart or something fun after the meal, like a favourite book. Make sure the goals you choose for your child are achievable for them.
Do not force feed them
To 30/45 minutes and snack times to 15 /20minutes
Make sure he/she has support under their feet, behind their back and they do not slip down too far in the seat – use non-slip mats if needed under feet and bottom.
Eat together as a family. Talk about the food in a positive way – make sure the food is the focus, not the child. You might want to use table cards as a
way of having conversations during meals that are not related to food only. We know that eating at the table can be extremely difficult for some children, so try changing sits at the table to avoid overwhelming situations
As well as new or less preferred foods – consider different plates or outside of their “safe area”
Enjoy eating and exploring your food – talk about the colours, textures, shapes, smells and sounds of the food. Encourage your child to think about these things too. Children learn by watching and copying.
For anything good they do, even if this is just touching or tasting a new
food. Some children don’t like to be praised, so avoid it.
Getting food on their hands and face is good for their learning. Clean up at the end. If your child is getting distressed during the meal, provide a napkin or small towel to wipe their hands.
Remember that is a new food and it might take few days/weeks for them to get used to it.
Remember that it is an exercise and your child is not expected to eat the food, it is about engaging and desensitizing them

Support Feeding At Home








Well Done!
- Completed

You have


My Notes
Supporting Videos

Looks aren't everything. Believe me, I'm a model.

Dove real beauty sketches. You're more beautiful than you think.

If you could change one thing about your body, what would it be?
We hear you and see you!
Get SupportSupported by










